Corneal Melt
All content on Eyewiki is protected by copyright law and the Terms of Service. This content may not be reproduced, copied, or put into any artificial intelligence program, including large language and generative AI models, without permission from the Academy.
Disease Entity
ICD-10 codes
- H16.0 Corneal ulcer
- H18.4 Corneal degeneration
Disease
Corneal melt, also known as keratolysis, is a pathologic process in which enzymatic degradation of corneal collagen and extracellular matrix leads to progressive stromal dissolution. In severe cases, corneal melt may result in descemetocele formation and eventual corneal perforation. It is commonly associated with infection, autoimmune disease, prior ocular surgery, and noxious topical ocular medication.
Epidemiology
Because corneal melt arises from diverse etiologies (see below), its overall incidence, prevalence, age, sex, and geographic distributions are not well defined. Epidemiologic information can be inferred from that of the underlying disease processes.
Etiology
Corneal melt may be idiopathic or a pathologic sequela to an underlying inflammatory process, such as:
- Infectious keratitis
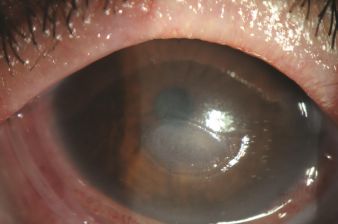 Figure 1. Anterior segment photo of a patient with Stevens-Johnson syndrome with corneal melting and associated haze. There is a semiflexible plastic ring around the cornea that previously held an amniotic membrane that has since dissolved. Photo courtesy of AAO Image Collection; © American Academy of Ophthalmology 202
Figure 1. Anterior segment photo of a patient with Stevens-Johnson syndrome with corneal melting and associated haze. There is a semiflexible plastic ring around the cornea that previously held an amniotic membrane that has since dissolved. Photo courtesy of AAO Image Collection; © American Academy of Ophthalmology 202

- Autoimmune disorders and hypersensitivity reactions
- Rheumatoid arthritis (most common systemic autoimmune disease associated with corneal melt, particularly when peripheral ulcerative keratitis is present)
- Psoriatic arthritis
- Graft versus host disease
- Sjögren syndrome[1]
- Systemic lupus erythematosus
- ANCA (anti-neutrophil cytoplasm antibodies)-associated vasculitides
- Stevens-Johnson syndrome (Figure 1)
- Chemical injury to cornea
- Topical NSAIDs, particularly diclofenac (melting may be exacerbated with concurrent use of topical steroids)[2][3]
- Topical anesthetic abuse keratopathy
- Alkali or acidic burns
- Thermal injury to cornea[4]
- Iatrogenic injury to cornea

Risk Factors
- Autoimmune/inflammatory disease, particularly rheumatoid arthritis
- Connective tissue disorder
- Trigeminal nerve dysfunction
- Facial nerve palsy
- Diabetes
- Contact lens wear
- History of herpes keratitis
- Chronic use of IOP-lowering drops
- Recent ocular surgery (particularly if intraoperative Mitomycin C or post-operative NSAIDs or 5-Fluorouracil were used)[3][5]
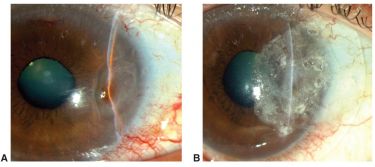 Figure 3. Slit-lamp photographs of corneal melting and perforation after nasal pterygium excision with conjunctival graft secured with tissue glue. A, Iris is attached to the perforation site with pupil distortion. B, Sealing of the perforation was performed with cyanoacrylate adhesive followed by application of bandage contact lens. Photo courtesy of Arie L. Marcovich, MD, PhD & AAO Image Collection; © American Academy of Ophthalmology 2026.
Figure 3. Slit-lamp photographs of corneal melting and perforation after nasal pterygium excision with conjunctival graft secured with tissue glue. A, Iris is attached to the perforation site with pupil distortion. B, Sealing of the perforation was performed with cyanoacrylate adhesive followed by application of bandage contact lens. Photo courtesy of Arie L. Marcovich, MD, PhD & AAO Image Collection; © American Academy of Ophthalmology 2026.

General Pathology
Corneal melt is a pathologic process characterized by excessive proteolytic degradation of stromal collagen and extracellular matrix that overwhelms normal corneal repair mechanisms. This derangement leads to progressive stromal thinning, descemetocele formation, and ultimately corneal perforation.
Pathophysiology
The corneal stroma is primarily composed of type I and IV collagen that are embedded within a proteoglycan-rich extracellular matrix. Under normal conditions, corneal homeostasis is maintained through a controlled balance of matrix production by keratocytes and extracellular matrix turnover tissue proteases.
In corneal melt, this balance is disrupted by excessive proteolytic activity. Upregulation of matrix metalloproteinases (MMPs) degrade stromal collagen and basement membrane components.[7][8][9] Additional proteolytic enzymes, including neutrophil-derived collagenases, elastases, cathepsins, and other serine proteases, contribute to stromal breakdown.[10][11][12] Tissue inhibitors of metalloproteinases (TIMPs) are endogenous inhibitors of proteolysis that normally prevent excess proteolysis. In corneal melt, TIMPs may be overwhelmed or deficient, resulting in unchecked extracellular matrix degradation.[13]
Inflammatory cells also play a role in disease progression. Neutrophils infiltrate the cornea and release inflammatory cytokines, which upregulate MMP production and exacerbate tissue destruction.[9][14]
As stromal dissolution progresses, the cornea loses structural integrity. In advanced disease, complete stromal loss with anterior protrusion of Descemet’s membrane forms a descemetocele. Rupture of the descemetocele results in corneal perforation.
Primary Prevention
Prevention of corneal melt should focus on reducing risk factors and controlling underlying autoimmune disease, ocular surface disease, or active corneal infection. Additionally, noxious topical medications in high-risk eyes should be used with caution or avoided altogether.
Diagnosis
History
When evaluating a patient with suspected corneal melt, a thorough medical and surgical history is essential. Clinicians should inquire about symptom onset, duration, and progression of symptoms.
Potential risk factors and underlying disease etiologies (see above) should also be clarified.
Medication history should include the use of any topical eye drops, with particular attention to topical NSAIDs, steroids, and glaucoma medications. Medication history should also clarify the use of any systemic immunosuppressive therapies.
Symptoms
- Decreased vision
- Ocular pain (neurotrophic cases may present with decreased pain or sensation)
- Redness
- Tearing
- Photophobia
Physical Examination
Evaluation of patients should include measurement of visual acuity, pupil reaction, intraocular pressure, corneal sensation, as well as examination of the eyes with a slit lamp. Ocular ultrasonography should be completed to evaluate the posterior segment of the eye if unable to view posteriorly with the slit lamp exam.

Signs
- Clear or purulent discharge
- Conjunctival injection
- Corneal epithelial defect
- Corneal stromal infiltrate
- Stromal thinning
- Stromal necrosis
- Descemetocele (Figure 4)
- Positive Seidel test or uveal prolapse if perforation occurs
- Cell or flare in anterior chamber
- Hypopyon
Clinical Diagnosis
Corneal melt is a clinical diagnosis based on examination findings. Ancillary testing is useful in determining whether there is an underlying etiology for the melt, and to rule out other corneal disease with similar presentation.
Diagnostic Procedures
Corneal scraping for cultures, smears, and viral nucleic acid amplification testing should be completed to assess whether an infectious etiology is present. Corneal biopsy should be considered in patients who are non-responsive to initial therapies, as well as in patients with concern for neoplasia.
A baseline anterior segment optical coherence tomography (OCT) should be completed to determine the extent of stromal thinning and risk of perforation.
Laboratory Testing
While there is no specific laboratory test to diagnose corneal melt, laboratory testing may be utilized to identify an underlying inflammatory condition. Depending on the suspected cause, relevant studies may include:
- Complete blood count (CBC)
- Complete metabolic profile (CMP)
- Rheumatoid factor (RF)
- Anti-cyclic citrullinated peptide antibody (anti-CCP)
- Antinuclear antibody (ANA)
- Antineutrophil cytoplasmic antibody (ANCA)
- Rapid plasma reagin (RPR)
- Chest x-ray
Differential Diagnosis
- Degenerative corneal conditions
- Inflammatory conditions
- Behçet disease
- Mooren's ulcer
- Stevens-Johnson syndrome (see Figure 1 above)
- Marginal keratitis
Management
General Treatment
The management of corneal melt is directed toward halting stromal degradation, preserving globe integrity, and identifying and treating the underlying etiology, if present. Treatment is typically escalated in a stepwise fashion based on the severity of the melt and its response to treatment.
Medical Therapy
Lubrication with preservative-free eye drops and ointments is important to maintain a moisture barrier and slow keratocyte loss. Autologous serum eye drops can be used in severe cases to promote stromal and epithelial healing.[15]
For suspected infectious etiology, topical or systemic antibiotics should be tailored to the inciting organism. Topical antibiotics can also be used for prophylaxis. Independent of its antimicrobial activity, doxycycline has been demonstrated to decrease inflammatory cytokines and matrix metalloproteinases and stabilize corneal melting.[16][17]
The use of topical steroids in the setting of infection is controversial, as there is debate to whether or not steroids improve long term healing and visual outcomes[18] (see Steroids for Corneal Ulcers Trial). The AAO recommends that the causative organism be identified before starting steroids; steroids should be delayed at least 24 hours after initiating antibiotics to ensure clinical response; and steroids should not be used at all in the setting of fungal, Acanthamoeba, or Nocardia infection.[19]
For non-infectious inflammatory etiologies, immunosuppressive and modulatory agents can be started to dampen the inflammation that drives the melting process. These agents are often used in a stepwise fashion, starting with corticosteroids, cyclosporine, methotrexate, or mycophenolate.[20][21] In aggressive or refractory cases, escalation to cyclophosphamide, rituximab, or infliximab may be necessary.[22][23][24] In the setting of systemic inflammatory conditions, working with rheumatology on medical management is advised.
Vitamin C can be used as an adjunct treatment to support collagen synthesis, particularly in corneal melt secondary to alkali burn injury.[25]
Topical NSAIDs should be avoided as they can exacerbate tissue destruction.[2][3] Topical anesthetics are also not recommended as they delay wound healing, mask worsening symptoms, and can be abused (see Topical Anesthetic Abuse Keratopathy).[26]
Surgery
Surgical treatment is indicated when medical therapy fails to halt stromal thinning, or when there is impending or complete corneal perforation.

Corneal surface protective methods such as bandage contact lens, amniotic membrane transplant, and tarsorrhaphy can be useful in non-infectious corneal melts to reinforce the cornea and protect from mechanical irritation from blinking, exposure keratopathy, or neurotrophic keratitis.[27]
Tissue adhesive with cyanoacrylate or fibrin glue can be used for small corneal perforations. A bandage contact lens is then placed over the glue. (Figure 5)
Corneal grafts should be considered for large melts or perforations. Depending on size and depth of melt, graft types include:
- Descemet Stripping Endothelial Keratoplasty (DSEK) or Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK)
In eyes with limited visual potential, a conjunctival flap can be considered as an alternative to keratoplasty.[32] A conjunctival flap provides structural reinforcement to the cornea as well as vascular supply to promote corneal healing.
Corneal cross-linking strengthens corneal stroma and has direct antimicrobial effects. It may be considered for superficial corneal melts, particularly if caused by an underlying infectious keratitis.[33][34]
Follow-Up
Patients with active corneal melt require frequent follow-up to monitor for progression of stromal thinning, descemetocele formation, perforation, infection, and response to therapy. Follow-up intervals may range from daily to monthly depending on acuity.
Long-term management should focus on controlling the underlying disease process and optimizing ocular surface health to prevent recurrence. For autoimmune-associated corneal melt, close collaboration with rheumatology is often necessary.
Post-operative patients should be monitored closely for recurrence of disease, infection, and graft rejection.
Anterior segment OCT imaging should be repeated periodically at follow-up visits to monitor disease regression versus progression.
References
- ↑ Brejchova K, Liskova P, Hrdlickova E, Filipec M, Jirsova K. Matrix metalloproteinases in recurrent corneal melting associated with primary Sjörgen’s syndrome. Mol Vis. 2009;15:2364. Accessed June 10, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC2779063/
- ↑ 2.0 2.1 Rigas B, Huang W, Honkanen R. NSAID-induced corneal melt: Clinical importance, pathogenesis, and risk mitigation. Surv Ophthalmol. 2020;65(1):1-11. doi:10.1016/j.survophthal.2019.07.001
- ↑ 3.0 3.1 3.2 Cabourne E, Lau N, Flanagan D, Nott J, Bloom J, Angunawela R. Severe corneal melting after cataract surgery in patients prescribed topical postoperative NSAIDs and dexamethasone/neomycin combination therapy. J Cataract Refract Surg. 2020;46(1):138-142. doi:10.1016/J.JCRS.2019.08.033
- ↑ 4.0 4.1 Yang Z, Wang YQ, Wang Q, et al. Causes of Corneal Melt After the Boston Keratoprosthesis Type I: The Chinese People’s Liberation Army General Hospital Experience. Cornea. 2024;43(8):936-941. doi:10.1097/ICO.0000000000003563
- ↑ Ando H, Ido T, Kawai Y, Yamamoto T, Kitazawa Y. Inhibition of Corneal Epithelial Wound Healing: A Comparative Study of Mitomycin C and 5-Fluorouracil. Ophthalmology. 1992;99(12):1809-1814. doi:10.1016/S0161-6420(92)31721-X
- ↑ Chan CC, Loverde L, Qiang J, Nordlund ML, Holland EJ. Incidence, risk factors, and surgical management of boston type 1 keratoprothesis corneal melts, leaks, and extrusions. Cornea. 2016;35(8):1049-1056. doi:10.1097/ICO.0000000000000911
- ↑ Sakimoto T, Sawa M. Metalloproteinases in corneal diseases: degradation and processing. Cornea. 2012;31 Suppl 1(11 SUPPL.1). doi:10.1097/ICO.0B013E318269CCD0
- ↑ Brejchova K, Liskova P, Cejkova J, Jirsova K. Role of matrix metalloproteinases in recurrent corneal melting. Exp Eye Res. 2010;90(5):583-590. doi:10.1016/J.EXER.2010.02.002
- ↑ 9.0 9.1 García-López C, Rodríguez-Calvo-de-Mora M, Borroni D, Sánchez-González JM, Romano V, Rocha-de-Lossada C. The role of matrix metalloproteinases in infectious corneal ulcers. Surv Ophthalmol. 2023;68(5):929-939. doi:10.1016/j.survophthal.2023.06.007
- ↑ Zhu Y, Huang Y, Ji Q, et al. Interplay between Extracellular Matrix and Neutrophils in Diseases. J Immunol Res. 2021;2021(1):8243378. doi:10.1155/2021/8243378
- ↑ Kettritz R. Neutral serine proteases of neutrophils. Immunol Rev. 2016;273(1):232-248. doi:10.1111/IMR.12441;WGROUP:STRING:PUBLICATION
- ↑ Lin M, Jackson P, Tester AM, et al. Matrix metalloproteinase-8 facilitates neutrophil migration through the corneal stromal matrix by collagen degradation and production of the chemotactic peptide pro-gly-pro. American Journal of Pathology. 2008;173(1):144-153. doi:10.2353/ajpath.2008.080081
- ↑ Sakimoto T, Ohnishi T, Ishimori A. Simultaneous study of matrix metalloproteinases, proinflammatory cytokines, and soluble cytokine receptors in the tears of noninfectious corneal ulcer patients. Graefes Arch Clin Exp Ophthalmol. 2014;252(9):1451-1456. doi:10.1007/S00417-014-2708-1
- ↑ Folorunso OS, Sinha NR, Singh A, et al. Tissue Inhibitor of Metalloproteinase 2 Promotes Wound Healing by Suppressing Matrix Metalloproteinases and Inflammatory Cytokines in Corneal Epithelial Cells. American Journal of Pathology. 2025;195(4):754-769. doi:10.1016/j.ajpath.2024.11.007
- ↑ Shtein RM, Shen JF, Kuo AN, Hammersmith KM, Li JY, Weikert MP. Autologous Serum-Based Eye Drops for Treatment of Ocular Surface Disease: A Report by the American Academy of Ophthalmology. Ophthalmology. 2020;127(1):128-133. doi:10.1016/j.ophtha.2019.08.018
- ↑ McElvanney AM. Doxycycline in the management of pseudomonas corneal melting: two case reports and a review of the literature. Eye Contact Lens. 2003;29(4):258-261. doi:10.1097/01.ICL.0000086490.38331.58
- ↑ Bian F, Pelegrino FSA, Henriksson JT, et al. Differential Effects of Dexamethasone and Doxycycline on Inflammation and MMP Production in Murine Alkali-Burned Corneas Associated with Dry Eye Presented in part as abstracts at the annual meeting of the Association for Research in Vision and Ophthalmol. Ocular Surface. 2016;14(2):242-254. doi:10.1016/j.jtos.2015.11.006
- ↑ Sharma B, Soni D, Mohan RR, et al. Corticosteroids in the Management of Infectious Keratitis: A Concise Review. J Ocul Pharmacol Ther. 2021;37(8):452-463. doi:10.1089/JOP.2021.0040
- ↑ Rhee MK, Ahmad S, Amescua G, et al. Bacterial Keratitis Preferred Practice Pattern®. Ophthalmology. 2024;131(4):P87-P133. doi:10.1016/j.ophtha.2023.12.035
- ↑ Knox Cartwright NE, Tole DM, Georgoudis P, Cook SD. Peripheral ulcerative keratitis and corneal melt: a 10-year single center review with historical comparison. Cornea. 2014;33(1):27-31. doi:10.1097/ICO.0000000000000008
- ↑ Kervick GN, Pflugfelder SC, Haimovici R, Brown H, Tozman E, Yee R. Paracentral Rheumatoid Corneal Ulceration: Clihical Features and Cyclosporine Therapy. Ophthalmology. 1992;99(1):80-88. doi:10.1016/S0161-6420(92)32006-8
- ↑ Guindolet D, Reynaud C, Clavel G, et al. Management of severe and refractory Mooren’s ulcers with rituximab. Br J Ophthalmol. 2017;101(4):418-422. doi:10.1136/BJOPHTHALMOL-2016-308838
- ↑ Forestier MG, Calderón RM, Oliver A. An Overview of Rheumatoid Arthritis-Associated Dry Eye Disease, Scleritis, and Peripheral Ulcerative Keratitis. J Clin Med. 2026;15(9). doi:10.3390/JCM15093207
- ↑ Utine CA, Birlik M, Özizmirliler D, Karakaş A, Akbulut B, Durak I. TNF-α Inhibitors for the Management of Intractable Corneal Melt: Report of Three Cases and Review of the Literature. Eye Contact Lens. 2021;47(6):372-377. doi:10.1097/ICL.0000000000000770
- ↑ Pfister RR, Haddox JL, Yuille-Barr D. The combined effect of citrate/ascorbate treatment in alkali-injured rabbit eyes. Cornea. 1991;10(2):100-104. doi:10.1097/00003226-199103000-00002
- ↑ Lee MD, Driver TH, Seitzman GD. Cornea Specialists Do Not Recommend Routine Usage of Topical Anesthetics for Corneal Abrasions. Ann Emerg Med. 2019;74(3):463-466. doi:10.1016/j.annemergmed.2019.04.016
- ↑ Dang DH, Riaz KM, Karamichos D. Treatment of Non-Infectious Corneal Injury: Review of Diagnostic Agents, Therapeutic Medications, and Future Targets. Drugs. 2022;82(2):145-167. doi:10.1007/S40265-021-01660-5
- ↑ Ke L, Shen D, Wang H, Qiao C, Zeng Q. Lamellar Keratoplasty Combined with Amniotic Membrane Transplantation for the Treatment of Corneal Perforations: A Clinical and In Vivo Confocal Microscopy Study. Biomed Res Int. 2020;2020(1):7403842. doi:10.1155/2020/7403842
- ↑ Suzuki T, Yamaguchi T, Tomida D, Fukui M, Shimazaki J. Outcome of Lamellar Graft Patching for the Treatment of Noninfectious Corneal Perforations. Cornea. 2022;41(9):1122-1128. doi:10.1097/ICO.0000000000002926
- ↑ Kusumesh R, Kishore A, Venugopal A, Shah SG, Vanathi M. Clinical application and outcome of Tenon’s patch graft: A comprehensive review. Indian J Ophthalmol. 2024;72(12):1714-1720. doi:10.4103/IJO.IJO_783_24
- ↑ Kate A, Vyas S, Bafna RK, Sharma N, Basu S. Tenon’s Patch Graft: A Review of Indications, Surgical Technique, Outcomes and Complications. Semin Ophthalmol. 2022;37(4):462-470. doi:10.1080/08820538.2021.2017470
- ↑ Singhal D, Nagpal R, Maharana PK, et al. Surgical alternatives to keratoplasty in microbial keratitis. Surv Ophthalmol. 2021;66(2):290-307. doi:10.1016/J.SURVOPHTHAL.2020.08.004
- ↑ Said DG, Elalfy MS, Gatzioufas Z, et al. Collagen cross-linking with photoactivated riboflavin (PACK-CXL) for the treatment of advanced infectious keratitis with corneal melting. Ophthalmology. 2014;121(7):1377-1382. doi:10.1016/j.ophtha.2014.01.011
- ↑ Davis SA, Bovelle R, Han G, Kwagyan J. Corneal collagen cross-linking for bacterial infectious keratitis. Cochrane Database Syst Rev. 2020;6(6). doi:10.1002/14651858.CD013001.PUB2